
Mini Review Article | DOI: https://doi.org/10.31579/2578-8868/117
1* ABC (American British cowdray) medical center Mexico city
*Corresponding Author: Carlos Francisco Gutierrez Partida, Neurosurgeon in Mexico City, Mexico.
Citation: Gutierrez Partida CF., Velazquez Aleman AP., (2020) XLIF MISS literature Review. J. Neuroscience and Neurological Surgery. 6(3); DOI:10.31579/2578-8868/117
Copyright: © 2020 Carlos Francisco Gutierrez Partida, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 13 February 2020 | Accepted: 03 March 2020 | Published: 19 March 2020
Keywords: XLIF; laterla interbody fusion
The interest to decrease the complications and morbility in patients, encourage the investigation to search for minor invasvies surgical techniques. The medical responsability for the wellness of the patient adds to the actual advanced technologies that is the origin to propose more efficent interventions. An example is the XLIF (extreme laterla interbody fusion) represents one of the avant-gard techniques of spine surgery. The XLIF represents an excelent option for the treatment of some spine compelx pathologies that needs descompression, balance alignement, arthrodesis and stabilization: degenerative disc disease, spondylolisthesis grade l and ll, deformities like degenerative scoliosis or adjacent disc disease are examples where the benefit of this technicc is evident. The XLIF represents an excelent option for the treatment of some spine compelx pathologies that needs descompression, balance alignement, arthrodesis and stabilization: degenerative disc disease, spondylolisthesis grade l and ll, deformities like degenerative scoliosis or adjacent disc disease are examples where the benefit of this technicc is evident. However, this method is contraindicated for L5-S1 (limited by iliac crest) disc disease or spondylolisthesis grade lll for example. [15]
The interest to decrease the complications and morbility in patients, encourage the investigation to search for minor invasvies surgical techniques. The medical responsability for the wellness of the patient adds to the actual advanced technologies that is the origin to propose more efficent interventions. An example is the XLIF (extreme laterla interbody fusion)) represents one of the avant-gard techniques of spine surgery. Developed by Luiz Pimenta in 2001 [1], this procedure offers the advantage to log into the lateral face of the lumbar spine trough small incisions that will avoid a damage in the paraspinal muscles. Obtained results are similars compared with the traditional techniques (intersomatic fusion). A similar endoscopic retroperitoneal technic was used at the beginnin without the expected success [11].
The XLIF represents an excelent option for the treatment of some spine compelx pathologies that needs descompression, balance alignement, arthrodesis and stabilization: degenerative disc disease, spondylolisthesis grade l and ll, deformities like degenerative scoliosis or adjacent disc disease are examples where the benefit of this technicc is evident. However, this method is contraindicated for L5-S1 (limited by iliac crest) disc disease or spondylolisthesis grade lll for example. [15]
The aim of the present work is to exposed the achieves of the aplication of this procedure, to explain some of the elemental features that this method needs and show the benefits than the technique offers. Likewise, the results like fusion rate, surgery time, bleeding and in-hospital stay needs to analize.
There are 5 basic principes of this technic that we need to keep in mind: The “ perfect lateral” position of the patient (Figure l), the gentil rertorperitoneal disection, the way through the psoas with neurophysiological monitoring, the complete resection of the disc with contralateral descompression of the annulus (Figure lll) and the apropiate size of the implant . It´s imperative the anatomic knowledge of the trans- psoas lateral extremity access, learn the relations of the muscular, visceral, vascular and nervous structures. The knowledge of this facts, decrease the surgical risks.

It is essential fot the procedure to recognize the muscular anatomy for a secure intervention. For learning purposes and a better understaning, it discriminates a superficial level and deep level. The superficial level is composed by external oblique, internal oblique and transversal oblique. The deep level conforms by psoas major and quadratus lumborum. The lumbar plexus is composed by the branches L1 to L4, they conforms a retroperitoneal structure and the fibers across among Psoas. It is required to avoid lesions to know the exact location of there structures. [2]
Takamoto Moro and collaborators [10], performed an anatomic study in corpses with the goal to recognize the safety areas of the lumbar plexus regarding the Psoas. They concluded than this safety area it is above of L2-L3. Right genitofemoral nerve has a path among the area ll, left genitofemoral nerve has a path among number lll, while the others nervous branches are in the number lV. In the flow rates levels the safety areas decrease.
Wan-Kun Hu, i etal. [8] dentified the relation among the Psoas with the great vessels. They place the vena cava in the area l toward the right flank. To the left, the aorta´s path it´s front at the area l. Are stabilshed as safety areas, for the levels L1-L2, L2-L3, both in left flank and right flank, the area ll and lll. For the levels L3-L4 the safety area it´s the number ll. In the level L4-L5 the safety area it´s number l for the left flank and the number l for the right flank.
It its important to know that this studies shows static structures, because this techniques was performed in cadavers. It is necesary to be aware the changes than the diferents positions of the patiens among the retroperitoneal structures. Armen R., etal. [14] performed a study where they evaluated, through magnetic resonance, the movements of the abdominal structrues regarding the position. The investigation include the right lateral decubitus and the left lateral decubitus; it proved than the aorta and the cava are located in a posterior flat at level L3-L4 and the kidneys are in caudal situation.
To recognize the safety areas described in the literature are fundamental for avoid injuries of the lumbar plexus and vascular structures. Likewise, neurophysiology monitoring is essential to avoid lessions. Bergey and collaborators [4] reported a rate of elevated complications compared with the procedures than used the monitoring adequately [5]. The electromyography constitutes the most appropriate monitoring, because the visualization of the lumbar plexus is complicated eventhoug in open techniques. The real time monitroing gives a posibility to keep safe the lumbar plexus, every time that it let us recognize indirectly. It is worth to mention that there are specific anesthetics to make adequtly the electrophysiology monitoring; the muscle relaxants should be avoid and removed by the patient´s metabolism when the monitoring started to avoid misunderstanding of the electrical impulse transmision lecture.
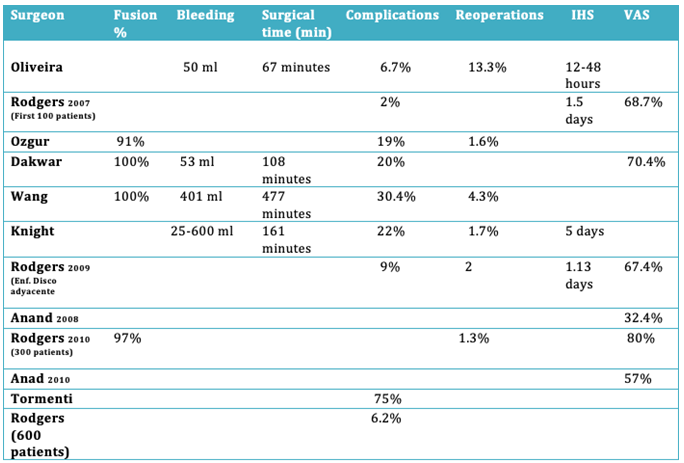
The results showed for diferents authors make evident a fusion rate for this procedure of 91%. Reported by Ozgur etal- of 100% reported by Dakwar etal-. The surgical time oscillate from 67 minutes- Oliveria etal.- to 477 minutes- Wang Etal.-. The amount of bleeding presented by patients oscillate from 50 ml- Oliveira, etal.- to 600 ml.- Knight, etal-. The complications oscillate from 2%- Rodgers, etal.- to 75%- Tormenti and collaborators. The in-hospital stay reports a minimum of 12 hours- Oliveira, etal.- to maximum of 5 days.- Knight, etal. With a improvement of the analogous visual scale until 80%- Rodger, etal.
Among the adventages it presents this technich are of biomechanics considerations. The removal of many intervertebral disk makes possible the placement of large implants. That proviedes a greater exposure surface form the implant to the platforms advantaged major fusion rates. This technique preserves anterior an posterior osteoligamentary structures that a substantial stability of the segment, sagittal and coronal correction coronal [6,7]. Vamivanij, etal. Remark a increase of 33% in the canal amplitude and a 41% in the foramen area product of the increase of the interdiscal space. Indirectly this technique auspicious the descompresion of the neural elements [8].
There are four posibilities to contribute to the fusion process: the called stand-alone lateral plaque, unilaterla transpedicular instrumentation or bilateral transpedicular instrumentation. Several studies analized this posibilities, however the results do not have statistical soundness since they have been carried out in non-homogeneous conditions. It is necesary a cautious analysis and new studies to provide truthful information. At the moment, research shows that bilateral instrumentation provides greater stiffness and biomechanical stability [7,9].
Thereffore, this technique provide notables advantages than other procedures as long as you have the precise comprehension of the anatomic and essentially the lumbar plexus. It is necesary to know the methods that better adjust to the patient accomodation to established an adequate management of the neurophysiological monitoring and to know specific crtieria of the preventive care. Altough, even in experience hands there are morbidity, that is the reason it is very important to know exactly the aspects of this procedure to accomplish with optimum results and secure.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
